February 10, 2020
Case Report: Using the Armeo®Spring in Upper Limb Functional Recovery Following Burn Injuries

Jean Baptiste Fauconnier, OT (first from the left in the background) with the occupational therapy team and two physicians.
Jean Baptiste Fauconnier, OT,
Léon Bérard Hospital, Hyères, France
We would like to share our clinical experience with a patient who suffered burn injuries. Mr. B. had an accident at home which induced severe burns of the left hemi-thorax and upper limb resulting in limitations in activities of daily living (ADL) and decreased overall quality of life. Upon admission, he was enrolled in our intensive rehabilitation program where he participated in individualized treatment including both multiple occupational and physical therapies, in order to regain functional independence. The patient’s experience with the intensive care and the positive outcomes motivated us to share how a combined approach of conventional therapies with the Armeo®Spring can be beneficial and how it can be incorporated into a program tailored for patients with burn injuries.
Pre-Treatment
Mr. B, 56 years old, was admitted with an ongoing wound-healing process on January 14, 2019 after a 2.5 month period in acute care following his accident at home early November 2018.
During his acute care, he underwent surgery consisting of excision & grafting and a left elbow skin-flap. Burn injuries covered 17% of his body surface area (chest and upper extremities), with his left upper extremity accounting for 5.5% (see Figure 1 and 2).
Prior to the accident, our patient lived independently in an apartment and conducted all ADL without any adaptive technologies.

Figure 1: Posterior view of burn injuries.

Figure 2: Frontal view of burn injuries.
His burn injuries resulted in functional impairments which noticeably impacted the level of performance in meaningful activities, and decreased his reported quality of life.
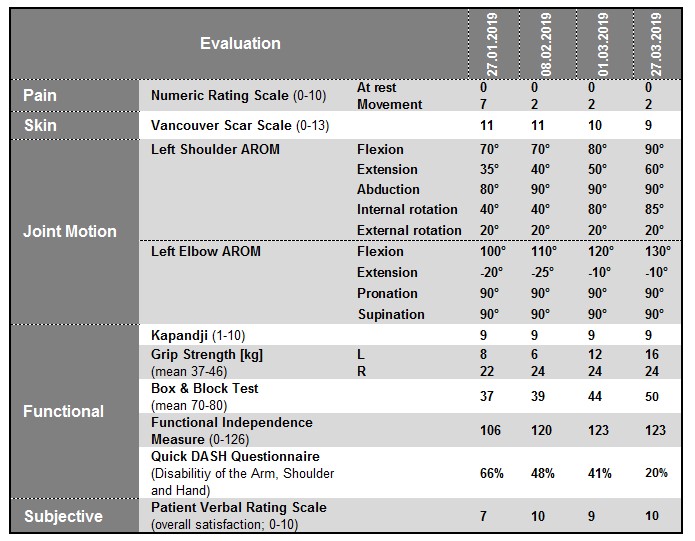
On January 27, our patient presented as follows (for detailed evaluation see Table 1):
- Pain in the affected areas while imoving or during activities
- Skin contractures in functional areas on left armpit and elbow crease
- Left upper extremity limitations (shoulder and elbow muscles weakness and joint deficits, Figure 5)
- Decreased left upper extremity gross motor coordination and postural control.
General therapy goals were:
- Increase range of motion (ROM)
- Increase muscle strength
- Improve functional movement abilities.
Treatment
Our patient followed a personalized rehab program for a total duration of 18 weeks.
The treatment included a combination of daily conventional occupational and physical therapy (30 min per session, 15 sessions per week) and ArmeoSpring sessions (20 min per session, 5 sessions per week).
Conventional therapy comprised stretching postures for the upper extremities and grasping exercises (fine and gross, distal and proximal).
The ArmeoSpring training started after two weeks of the program and lasted for 8 weeks. It specifically focused on activities in the following categories:
- Movement coordination: 50%
- ROM 2D and 3D: 25%
- ROM 1D: 5%
- Grasping function: 5%
- Miscellaneous (cognitive,…): 20%
The therapy program was composed of exercises targeting left shoulder and elbow movement combinations (flexion and extension; abduction and adduction; rotations). The exercise level of difficulty started from easy and was increased to medium following our patient’s progress.

Figure 3: Patient during an ArmeoSpring therapy session.
Our patient also followed a splinting protocol (Figure 4) consisting of a thoracic, shoulder and elbow splint, to stretch the skin contractures (8 hours per day, for 1 month). Additionally our patient wore compression garments (23 hours per day, to be continued up to 2 years).
Finally, prior to returning home, ADL-specific skills were trained using a grocery shopping simulator, a cooking task simulator and a 3-day autonomous stay in a training apartment.

Figure 4: Patient’s thoracic splint.
Outcomes
Our patient’s overall functional performance was assessed throughout the treatment in order to see the effectiveness of the therapy program.
Our patient showed a high level of volition. As a result he was very observant and effectively took part in daily sessions.
He showed improvements in active range of motion (AROM, Figure 5 & 6, Table 1), general muscle strength, grasp function, movement coordination, and velocity, and a decreased level of disability as measured with the DASH questionnaire of the affected extremity.
As a result of upper extremity motor improvement, our patient was rated higher on the Functional Independence Measure, showing an increased level of performance and independence in all activities of daily living which allowed him to return to home and live independently.

Figure 5: Limited hand-to-mouth movement capability at the beginning of the treatment.
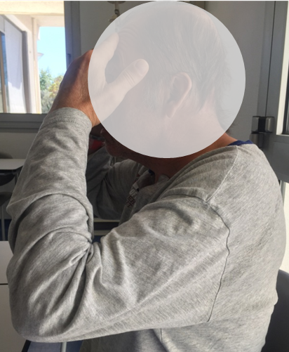
Figure 6: Effective hand-to-forehead movement at the end of the treatment.
Table 1: Initial and follow-up assessments of the patient.
Conclusion
The overall purpose of our case report was to address the effectiveness of adding ArmeoSpring to conventional occupational and physical therapy in a patient with burn injuries of the upper extremity. Our patient’s improvement and results suggest that conventional therapy in conjunction with daily ArmeoSpring sessions help promote faster recovery. The improvemements in terms of range of motion, strength, motor coordination, endurance and better integration of the impaired arm are beneficial for the patient’s overall levels of performance and therefore increase quality of life. Adding ArmeoSpring therapy sessions also seems to increase patient’s adherence to treatment plans.
On the other hand, while using the ArmeoSpring (and afterwards), we noticed no detrimental impact in terms of skin appearance, increased inflammatory state nor skin contracture.
We hope that our case study will inspire other therapists to add ArmeoSpring sessions to enhance their patients’ therapeutic outcomes.
About Us
Léon Bérard Hospital is a functional re-education and rehabilitation center located in the south of France (Hyères, Var), nested between Marseille and St. Tropez.
We have two inpatient units (257 beds) where we provide rehabilitative care for adult burn victims, orthopedics and trauma patients, as well as neuro and cardiovascular patients. On average, we have 2450 patients treated per year.
Our occupational therapy team consists of 9 occupational therapists and one head occupational therapist. In addition to conventional occupational therapy programs, we use the support of high-end equipment such as ArmeoSpring (2) and Armeo®Power (1), Andago® (1), computerized mirror therapy (1), driving simulator (1), training apartment (1), and a virtual reality headset (1).
![]()
This clinical experience report is meant to serve as an example of how the ArmeoSpring is integrated into the rehabilitation program of a patient suffering from burn injuries. It is not necessarily a standard recommendation from Hocoma.